CI and hearing aid – an interaction
About half the cochlear implant (CI) recipients use a hearing aid in the other ear. To ensure that these two different hearing systems work together well, the CI needs to replicate natural hearing.

In a talk at the 2010 Conference of the American Audiology Association US scientist Lisa Davidson stated that more than 50% of the children at her clinic were bimodal listeners, using a hearing aid in one ear and a CI in the other one. In 2016, research data from Hannover confirmed the high proportion of bimodal cochlear implant users in all age groups. Between 2010 and 2015 the number of bimodal listeners increased by almost 40%.
A German study delivered scientific proof for the benefits of bimodal hearing[1]: Bimodal benefit in quiet depends on hearing thresholds. Only if hearing thresholds in the second ear came close to CI candidacy, the bimodal benefits diminished. Subjects with better hearing on the acoustic side experienced more benefit from the bimodal condition.
Bimodality requires hearing aid and cochlear implant to be compatible with each other. “Many people think it’s just about streaming”, Jennifer Robinson, an experienced audiologist and project manager at MED-EL sighs. She has studied the potentials and challenges of bimodal hearing extensively. Two aspects are relevant, she explains: The implant system should simulate natural hearing as close as possible. And the signal processing used in the CI audio processor should match that of the hearing aid.
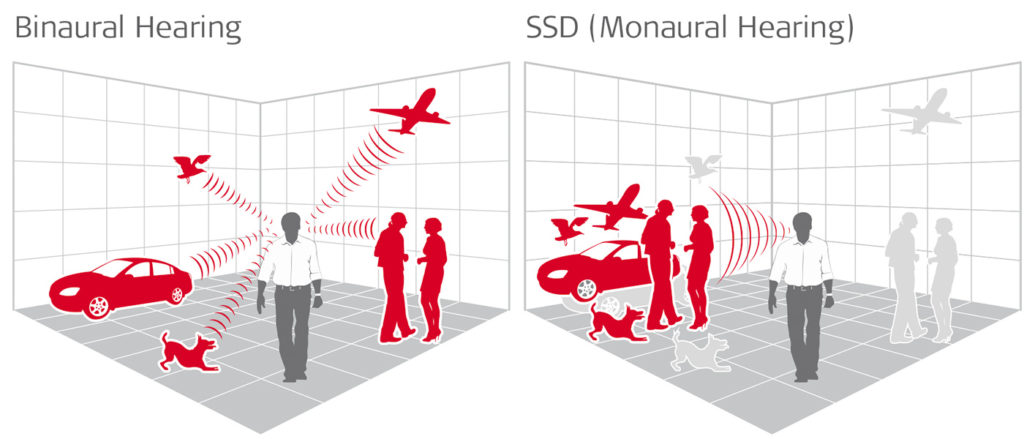
Binaural hearing delivers a more natural and richer hearing impression to CI users with single-sided deafness, bilaterally implanted CI users and bimodal recipients using hearing aid and CI.
Simulating natural pitch coding
Hearing aids amplify sound which, as a consequence, can be processed more easily by the inner ear. In contrast, the cochlear implant stimulates the hearing nerve directly, thereby replicating the function of the inner ear. The closer and more natural this replication is done, the better the hearing impression can be combined with the acoustic hearing on the other side (the so-called contralateral side). Therefore, both the implant’s frequency and temporal coding should resemble natural hearing.[2]
This requires a long electrode that can be fully inserted into the cochlea. One that covers its entire length and can therefore stimulate the inner ear at the corresponding places for high and low pitches.[3] Worldwide, currently only one implant manufacturer is offering this: MED-EL.
The importance of time differences
To perceive low pitches naturally, the time coding of sound is important.[4] It describes the detailed temporal analysis of the incoming audio signal. The hair cells transmit the nerve impulse at a clearly defined moment of the acoustic vibration. This exact temporal structure information can currently only be delivered by one CI system on the market: the MED-EL SYNCHRONY. Its fine structure coding in combination with its long, atraumatic electrode, which are both part of the Triformance technology, replicates the time coding of natural hearing. Fast processing of both systems avoids delays and allows simultaneous hearing in both ears.
Another important temporal aspect of hearing is based on the inner ear’s micro-mechanics. The movements of the travelling wave, which carries sound from the base of the inner ear to its apex, causes high frequencies to arrive just milliseconds before low frequencies in the tip of the cochlea. “We are the only CI manufacturer to consider this temporal delay”, Robinson explains proudly, referring to a [5]German comparison study that underlines her statement. “With our stimulation we are very close to natural hearing.”
Adapting loudness
The signal processing used in audio processors plays a vital role for binaural listeners. Only features that are available in both the hearing aid and the audio processor should be used. Audiologists and CI engineers need to take this into account during fitting.
One particularly important feature in both devices is called dynamic compression. A fully functional inner ear is about three times more sensitive to soft sounds than to loud sounds. The cochlear’s amplifying function for soft sounds progressively deteriorates in individuals with hearing loss. Hearing aid manufacturers try to compensate this natural feature in their devices.
MED-EL is so far the only manufacturer to implement this natural amplification with a 3:1 ratio and a possible variant of 2:1 up to 3.5:1 in their audio processors, while at the same time using the same place match as the normal hearing ear. MED-EL audio processors use a dynamic range close to that of the fully functional inner ear[6] and one that is similar to that of modern hearing aids. This is why MED-EL CI systems perfectly complement any conventional hearing aid on the contralateral ear – without requiring special coupling of the two devices.
Finally, the overall loudness of both devices needs to be fine-tuned to each other. Studies have demonstrated that the hearing aid should ideally be equally loud or slighly softer than the CI system.[7]
Assistive devices for both systems
Assistive listening devices should be compatible with the audio processor and the hearing aid. Induction loops are suitable for hearing aids as well as for audio processors with induction ports. They grant recipients independence from hearing aid and implant manufacturers.
For bimodal listeners, many universal assistive listening devices and communication systems, e.g. by Oticon or Phonak, are available to stream audio via Bluetooth. Phonak’s Roger system offers induction as well as direct input to audio processors and hearing aids.
Learning from Cinderella
We have learned one important thing from Cinderella: If you want to have a new shoe, don’t cut off your toe, for the shoe will still be too small. For bimodal hearing this means: if you choose and fit your hearing aid on the basis of your contralateral audio processor, some hearing potential will likely be lost in the hearing aid ear.
Type, function, fitting – there’s endless variations of hearing aids that make finding the ideal device and perfect fit for your individual hearing situation cumbersome. CI candidates often have had long-term hearing aid experience and are satisfied with the device that has met their individual needs for many years. A change may lead to long periods of readjustment and often comes with considerable costs. It is therefore essential to combine an optimally fitted hearing aid with a CI system that uses natural sound coding principles. This is MED-EL’s philosophy.
An optimally fitted CI system that can be combined with any hearing aid brand will ensure long-term hearing success. And this CI will lay the foundation for hearing success even when the contralateral hearing deteriorates and a second CI should be considered.[8] Audiologist Jennifer Robinson remarks: “If a CI is indicated in both ears, bilateral cochlear implantation is certainly the best choice.”
[1] Hoppe U., Hocke T., Digeser F. (2018) Bimodal benefit of cochlear implant listeners with different grades of hearing loss in the opposite ear, Acta Oto-Laryngologica, 138:8, 713-721, DOI: 10.1080/00016489.2018.1444281
[2] Wess JM, Brungart DS, Bernstein JGW (2017 May/Jun) The Effect of Interaural Mismatches on Contralateral Unmasking With Single-Sided Vocoders, Ear & Hearing, 38(3)374-486. Doi: 10.1097/AUD.0000000000000374
[3] Buchman C.A., Dillon M.T., King E.R., Adunka M.C., Adunka O.F. (2014) Pillsbury H.C., Influence of Cochlear Implant Insertion Depth on Performance: A Prospective Randomized Trial, Otology&Neurotology 35:1773-1779
[4] Rader, T., Döge, J., Adel, Y., Weissgerber, T., & Baumann, U. (2016). Place dependent stimulation rates improve pitch perception in cochlear implantees with single-sided deafness. Hear Res., 339, 94–103.
[5] Zirn S., Angermeier J., Arndt S., Aschendorff A, Wesarg T., 2019, Reducing the Device Delay Mismatch Can Improve Sound Localization in Bimomdal Cochlear Implant/Hearing-Aid Users, Trends in Hearing Volume 23: 1-13, DOI: 10.1177/2331216519843876, journals.sagepub.com/home/tia
[6] Plack CJ, Oxenham AJ (2000) Basilar-membrane nonlinearity estimated by pulsation threshold, J. Acousti. Soc. Am. 1063-7834/2000/107(1)
Vaerenberg B. et al, 2014, A Uniform Graphical Representation of Intensity Coding In Current-Generation Cochlear Implant Systems, Ear Hear 2014 Sep-Oct;35(5):533-43. Doi: 10.1097/AUD.0000000000000039.
[7] Dorman M.F., Loizou P., Wang S., Zhang T., Spahr T., Loiselle L., Cook S., Bimodal cochlear implants: The role of acoustic signal level in determining speech perception benefit, Audiol Neurootol. 2014; 19(4): 234-238, doi: 10.1159/000360070
[8] Gifford R.H., Driscoll C.L.W., Davis T.J., Fiebig P., Micco A., Dorman M.F., A within-subjects comparison of bimodal hearing, bilateral cochlear implantation, and bilateral cochlear implantation with bilateral hearing preservation: High-performing patients, Otol Neurotol. 2015 Sep; 36(8): 1331-1337. Doi: 10.1097/MAO.0000000000000804;
Gifford, R. and Dorman, M. (2018) Bimodal Hearing or Bilateral cochlear Implants? Ask the Patient” Ear Hear 2019 May/Jun;40(3):501-516. Doi: 10.1097/AUD.0000000000000657