Why you should always upgrade to the latest audio processor!
Today’s audio processors offer more than just a fresh design – they make a real difference to your listening experience. Find out here why a cochlear implant audio processor upgrade pays off and how easy it works.
MED-EL

In 1977, Prof. Dr. Kurt Burian used a cochlear implant for a deaf patient at the Vienna University Hospital (AKH). Since then, the implants have continuously evolved. Parallel to the implants, the audio processors have also been repeatedly adapted to the current state of the art technology. Innovative coding strategies and so-called adaptive intelligence, direction-dependent microphone systems and noise suppression enable an increasingly natural listening experience.
Latest technology – no matter how old the implant is
A cochlear implant audio processor upgrade can significantly improve hearing performance with the CI system, from speech perception, to understanding and locating the sound source. Users report better sound quality and music enjoyment after an upgrade and are happy when the user friendliness increases again and again. In addition, older processors, as with all devices, are also more susceptible to repair, whereas a new device guarantees reliable and powerful hearing results.
Not only those who are receiving an implant for the first time or replacing their implant can benefit from further developments in implant technology. In order to benefit from the latest technical advances in audio processors, CI users only need to replace the processor itself, without any operation and effort! For example, users of MED-EL multi-channel cochlear implants implanted 20 or more years ago can always use the latest generation of processors. In Austria, such optimised listening is also possible for CI users regardless of income, because the Austrian health system supports the regular switch to current audio processors!
Listening with excellent design
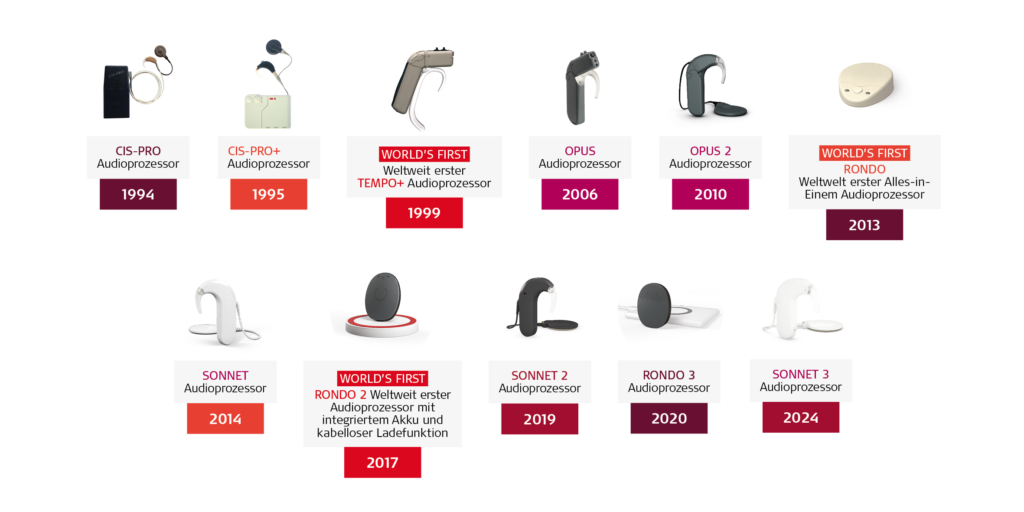
The first CI users listened through body-worn processors. Later, audio processors moved to the ear - similar to conventional hearing aids. Today, users can choose between these behind-the-ear audio processors or so-called single-unit audio processors, jokingly referred to by some users as a “hearing button.” The current model even won the Red Dot Design Award thanks to its innovative design!
In terms of energy supply, we can now choose between disposable batteries and rechargeable batteries. For example, the processors in the RONDO series, which was introduced in 2013, initially worked with conventional button cells, with the current RONDO 3, the battery is already integrated and can be charged wirelessly. In English, this type of processor is called "off-the-ear". this describes both the typical wearing position slightly behind and above the ear and the advantage of a free ear. The fact that a single-unit processor is in one piece, without cables, is another advantage.
Design & functionality: more than aesthetics
In addition, users can now not only choose from different colour options for their audio processor, but also change different design covers as desired. The protection against the ingress of moisture or dust also improved from one device generation to the next. Modern design can improve wearing comfort and avoid the often feared stigma of visible hearing care, but that would hardly be a reason for the health insurance company to finance the switch to a new device. For them, it is crucial that the inner components of the audio processors have also developed, which has a positive effect on speech comprehension even in difficult everyday situations.
Better listening with newer technology
Thanks to advanced coding strategies and features, new generations of processors enable even experienced CI users of all ages to enjoy far-reaching audiological benefits: from improved speech perception to better sound localisation, better sound quality, more music enjoyment and a more natural listening experience. Current audio processors also offer further improved handling and also enable users to stay at the cutting edge of time even when connecting various hearing aids and audio devices - just think of modern streaming options!
Why an upgrade makes everyday listening easier
CI users who had previously used Tempo+ for digital multi-channel CIs from MED-EL with the first behind-the-ear processor were able to benefit from the completely new signal coding of the OPUS 2 from 2006, from HD-CIS and especially from the FineHearing strategy. Numerous scientific studies soon showed that improvements in all areas of hearing and speech understanding could be achieved with the change. When the same CI users switched to SONNET or SONNET 2 in 2014, they gained a direction-dependent microphone system, interference suppression and adaptive sound processing, and again achieved improvements in hearing and understanding[1],[2],[3],[4],[5].
Similar improvements can also be expected in the processor upgrades for other implant types, e.g. EAS, BONEBRIDGE, VIBRANT-SOUNDBRIDGE, or in conventional hearing aids. Since 2024, the latest SONNET 3 behind-the-ear processor in MED-EL CI systems has been inspiring users with additional integrated streaming, IP68 water resistance, a flexible ear hook and a practical sensor button. The RONDO 3 is currently a single-unit processor.

The current SYNCHRONY 2 cochlear implant system as well as the COMBI 40 system from 1994, whose implant is compatible with the latest audio processors ©MED-EL

Health system support
Study[6] data suggests that CI users should be able to switch to new processor technology at any stage of their life, regularly and at no additional cost, even if they are already managing well with the existing systems. Bilateral users should preferably switch their external devices on both sides at the same time in order to use the same signal processing on both sides. Numerous clinical guidelines[7],[8],[9],[10],[11],[12] - especially those of the CI expert group HEARRING[13] - recommend an upgrade interval of a maximum of five years. The recommendation is based on scientific publications.[14],[15],[16],[17]
In Belgium, an upgrade is possible every three years for children under eight, every five years for all other CI users. In France, CI users can upgrade free of charge every five years. In many countries, however, public health systems cannot offer such optimal opportunities. In some countries, upgrades may even have to be self-financed or at least subject to further conditions. On the other hand, there are unfortunately CI manufacturers whose latest audio processors are not necessarily compatible with all their implants. In Austria, we are now in the fortunate situation that the health insurance companies are financing an upgrade of the CI audio processors after at least seven years of use of the previous devices. As a CI manufacturer, MED-EL ensures that the current CI audio processors are always compatible with all MED-EL multi-channel cochlear implants. So you can benefit from the latest processor technology even if you received your MED-EL cochlear implant 20 years or more ago.
Take advantage of this opportunity for better listening and understanding, greater comfort and better compatibility with modern audio technology! Find out how easy it is to change a processor and what the current MED-EL processors offer at ZENTRUM HÖREN in Vienna, at MED-EL service partners or at your MED-EL CI technician.
Users can benefit from the latest processor technology even if they received their MED-EL cochlear implant 20 years or even longer ago. ©MED-EL
[1] Wimmer W, Weder S, Caversaccio M, Kompis M. Speech Intelligibility in Noise With a Pinna Effect Imitating Cochlear Implant Processor. Otol Neurotol 2016; 37(1): 19-23.
[2] Honeder C, Liepins R, Arnoldner C, et al. Fixed and adaptive beamforming improves speech perception in noise in cochlear implant recipients equipped with the MED-EL SONNET audio processor. PLoS One 2018; 13(1): e0190718.
[3] Kurz A, Zanzinger M, Hagen R, Rak K. The impact of cochlear implant microphone settings on the binaural hearing of experienced cochlear implant users with single-sided deficiency. Eur Arch Otorhinolaryngol 2021; 278(6): 2067-77.
[4] Kurz A, Rak K, Hagen R. Improved performance with automatic sound management 3 in the MED-EL SONNET 2 cochlear implant audio processor. PLoS One 2022; 17(9): e0274446.
[5] Muller V, Krause J, Klunter HD, Streicher B, Lang-Roth R. Speech perception in noise and sound localisation using different microphone modes in paediatric bilateral cochlear implant users. Int J Pediatr Otorhinolaryngol 2022; 156: 111117.
[6] Rauch AK, Metzner T, Aschendorff A, et al. [Speech processor upgrade increases speech comprehension in patients with cochlear implants]. Hno 2019; 67(10): 778-85.
[7] British Cochlear Implant Group. Quality Standards–Cochlear Implant Services for Children and Adults. Published in 2018–Reviewed in 2020. www.bcig.org.uk/_userfiles/pages/files/qsupdate2018wordfinalv2.pdf
[8] Cullington HE, Jiang D, Broomfield SJ, et al. Cochlear implant services for children, young people and adults. Quality standard. Cochlear Implants Int 2023: 1-13.
[9] ORL company AC-IdS. Guidelines for cochlear implant care and follow-up. Switzerland; 2018.
[10] Centene Corporation. United States. Clinical Policy: Cochlear Implants Replacement. Last review in 2019
[11] Government of Canada. 2.0 Audiology equipment and supplies benefits list. Effective April 18, 2023. www.sac-isc.gc.ca/eng/1585321635593/1585321656771#s2-3-3
[12] Department of Health WA. Clinical Guidelines for Adult Cochlear Implantation. Australia; 2013.
[13] https://www.hearring.com/quality-standards-collection/
[14] Muller J, Raine CH. Quality standards for adult cochlear implantation. Cochlear Implants Int 2013; 14 Suppl 2: S6-12.
[15] Martin J, Raine CH. Quality standards for cochlear implantation in children and young adults. Cochlear Implants Int 2013; 14 Suppl 2: S13-20.
[16] Hagen R. Quality standards for combined electric and acoustic stimulation. Cochlear Implants Int 2013; 14 Suppl 2: S27-33.
[17] Távora-Vieira D, Rajan G, Van de Heyning P, Mertens G. Quality standards for adult cochlear implantation in single-sided deficiency and asymmetric hearing loss. B-Ent 2021; 16(4): 209-16





